علاجات مختلفة لتصحيح الجنف
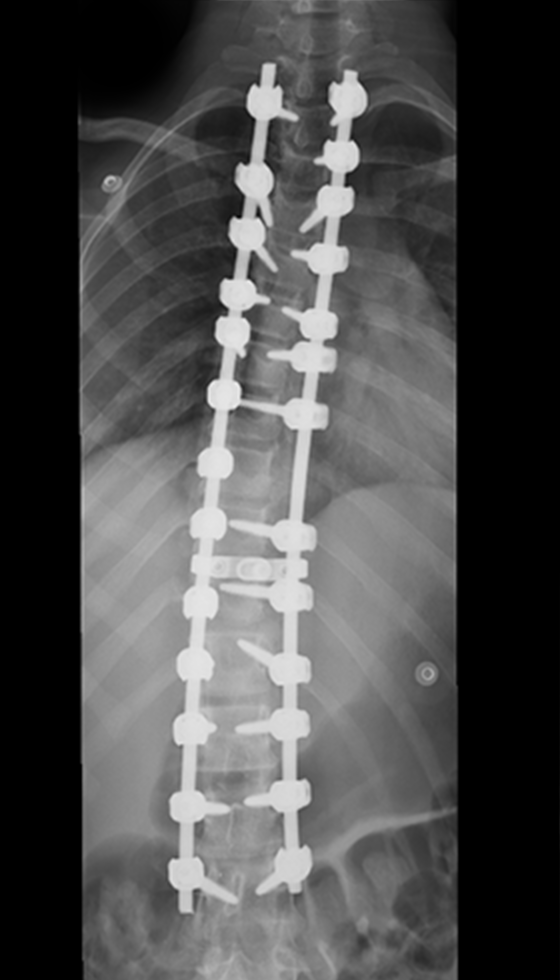
1. دمج الفقرات (تصحيح الجنف المعقد) - عادةً ما يكون
الانحناء شديداً / متفاقماً
يُعدّ دمج الفقرات الخيار الجراحي الأكثر شيوعاً
لعلاج الجنف، ويُنصح به عادةً في حالات الانحناءات
المتوسطة إلى الشديدة أو المعقدة، لا سيما عندما يتفاقم
الانحناء أو يؤثر على التوازن والوظائف الحركية.
وييتم اللجوء إلى هذا الإجراء غالباً عندما يصل
الانحناء إلى 45-50 درجة أو أكثر في العديد من
حالات المراهقين، وفي حالات الانحناءات الأكبر أو
المصحوبة بأعراض لدى البالغين (قد يختلف الحد
الأدنى المطلوب بحسب الحالة).
يتضمن الإجراء إعادة تموضع العمود الفقري وتثبيته
بمسامير وقضبان. ثم يتم وضع طعم عظمي بحيث
تلتئم الفقرات المعالجة تدريجياً لتشكل قطعة واحدة
صلبة. وهذا يخلق استقراراً طويل الأمد، ويمنع تفاقم
الانحناء، ويحسن المحاذاة العامة للعمود الفقري.
2. التصحيح المرن للجنف - انحناءات متوسطة مختارة
التصحيح المرن للجنف، هي تقنية طفيفة التوغل ولا
تعتمد على دمج الفقرات، تُستخدم في حالات مختارة
من الجنف لتحسين استقامة العمود الفقري مع الحفاظ
على حركة طبيعية قدر الإمكان. ويُنظر إليها عادةً في
حالات الانحناءات التدريجية والمرنة، والتي تتراوح
عادةً بين 30 و65 درجة لدى المرشحين المناسبين
(تختلف المعايير الدقيقة باختلاف الجراح وعوامل
المريض).
يتم إجراء هذه العملية من خلال عمل شقوق جانبية
صغيرة، حيث يضع الجراح مثبتات على طول جانب
الفقرات المنحنية ويربطها باستخدام حبل مرن. يُشد
الرباط برفق لتصحيح الانحناء ودعم توازن العمود
الفقري، مع الحفاظ على مرونته للمساعدة في الحفاظ
على الحركة.
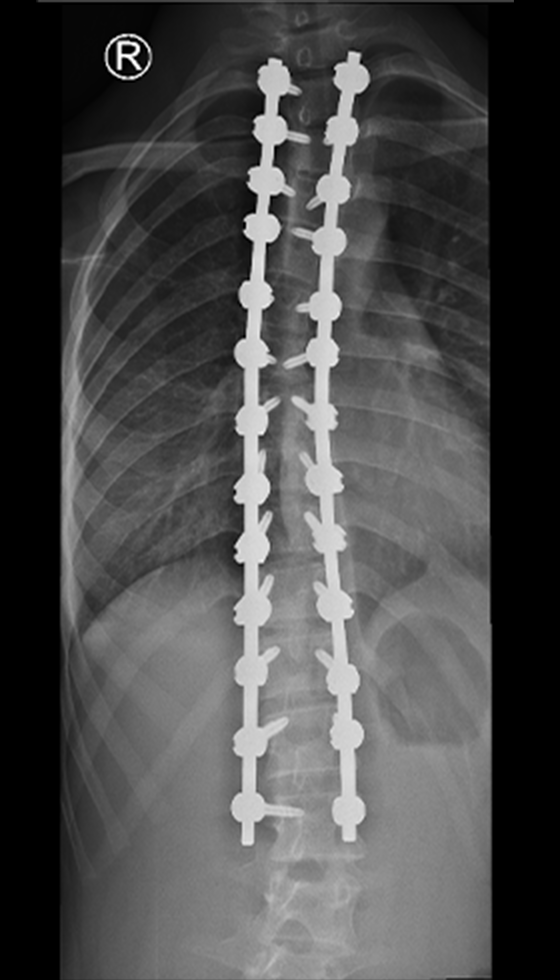
3. جراحة الجنف الهجينة (الدمج الخلفي للفقرات +
التصحيح المرن) - انحناءات مختلطة / معقدة
جراحة الجنف الهجينة هي نهجٌ مُدمج يجمع بين دمج
الفقرات لعلاج الجزء الأكثر صلابةً وتماسكاً من
انحناء العمود الفقري، وتطبيق تقنية التصحيح المرن،
لعلاج الجزء المجاور الأكثر مرونة. لا يُعد هذا
الخيار إجراءً روتينياً لجميع المرضى، بل يُنظر فيه
فقط في حالات مُحددة بعد تقييم شامل من قِبل
أخصائي. تشمل العوامل التي يتم تقييمها نمط
الانحناء، والمرونة كما تظهر في صور الأشعة
السينية أثناء الانحناء، والتوازن العام للعمود الفقري،
ونمو المريض أو نضج هيكله العظمي. تُعد مواعيد
المتابعة ضرورية لمراقبة استقامة العمود الفقري
بمرور الوقت.
فيما يلي النطاقات النموذجية لزاوية كوب (للإرشاد
العام؛ يتم تحديدها حسب الحالة):
- مكون الدمج (للانحناءات الهيكلية / الصلبة): غالباً
ما يتم النظر في هذه التقنية عندما يكون الانحناء
كبيراً، أي حوالي 45 درجة إلى 50 درجة أو أكثر،
خاصة إذا ما كان متطوراً، مما يسبب عدم التوازن،
أو يؤثر على الوظائف الحيوية للمريض أو مظهره.
- مكون الربط/التصحيح المرن (للانحناءات المرنة):
يتم النظر في هذه التقنية عادةً للانحناءات المرنة
والمتقدمة المختارة التي تتراوح قياساتها من 30
درجة إلى 65 درجة تقريباً، اعتماداً على مرونة
الانحناء ونوعه وحالة نمو المريض.
4. تصحيح الجنف طفيف التوغل - حالات مختارة من
الجنف الخفيف إلى المتوسط
يشير مصطلح تصحيح الجنف طفيف التوغل إلى
تقنيات جراحية تُجرى من خلال شقوق صغيرة
ومحددة في الظهر، باستخدام أدوات متخصصة وتقنية
تحافظ على العضلات، وذلك لتصحيح وتثبيت انحناء
العمود الفقري. يُنصح بهذا الإجراء عموماً لأنواع
محددة من الجنف، وغالباً ما يكون ذو انحناءات خفيفة
إلى متوسطة - عادةً ما بين 25 و45 درجة تقريباً،
وذلك بحسب درجة التعقيد والمرونة والخطة
الجراحية.
في حالات مختارة، يستطيع الجراح تثبيت العمود
الفقري وإجراء التصحيح اللازم مع تقليل تضرر
الأنسجة الرخوة، مما يدعم نهجاً يركز على التعافي.
وتعتمد ملاءمة هذه الطريقة على شكل الانحناء ومدى
تعقيده وتقييم الأخصائي.
5. قضبان النمو المتحكَّم بها مغناطيسياً (MCGR) -
منحنيات النمو المبكرة / التدريجية لدى المرضى في
طور النمو
توفر قضبان النمو المغناطيسية (MCGR) خياراً
مناسباً لنمو بعض المرضى الذين لا يزالون في طور
النمو ويحتاجون إلى التحكم في انحناء العمود الفقري
مع السماح لهم بمواصلة النمو. يُنصح عادةً باستخدام
القضبان المغناطيسية عندما يكون الانحناء متفاقماً
وكبيراً، وغالباً ما يصل إلى 40-60 درجة أو أكثر،
وخاصة في حالات الجنف المبكر حيث يكون الحفاظ
على النمو أمراً بالغ الأهمية (يختلف الحد الأدنى
حسب الحالة).
تُزرع قضبان على طول العمود الفقري لتوجيه النمو
والمساعدة في التحكم في الانحناء. ويمكن إطالتها
بطريقة غير جراحية خلال زيارات المتابعة باستخدام
جهاز تحكم مغناطيسي خارجي، مما يقلل الحاجة إلى
عمليات جراحية مفتوحة متكررة للإطالة، مع مراقبة
دقيقة على مدار الوقت.
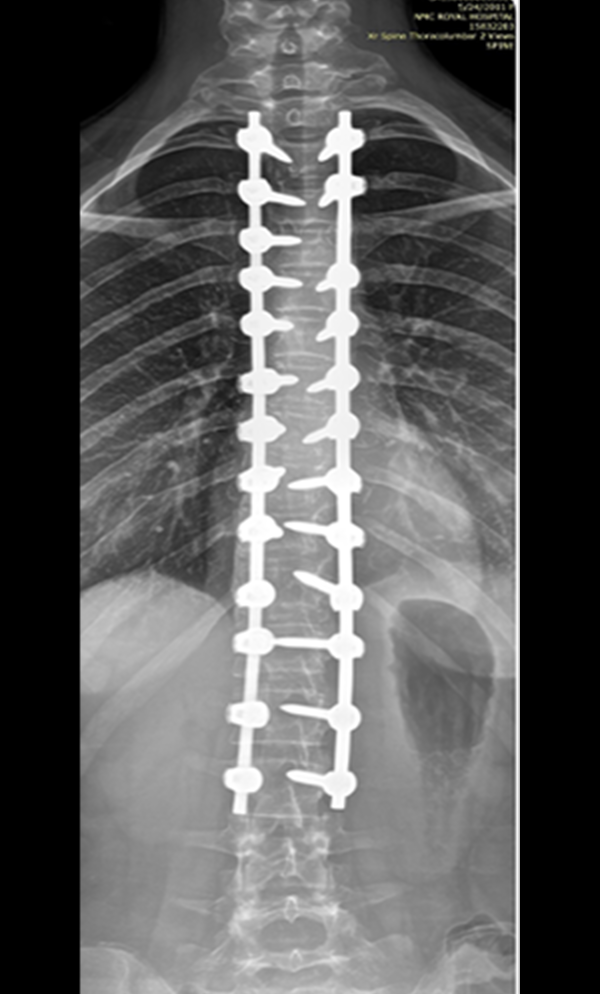
6. تصحيح قمة الجذر النشط (APC) - عادةً ما يكون
انحناءً شديداً / تدريجياً مبكر الظهور
يُعدّ تصحيح قمة العمود الفقري النشط (APC) تقنيةً
حديثةً غير جراحية، مصممة لتوجيه نمو العمود
الفقري في حالات مختارة من الجنف. الهدف
الأساسي هو التحكم في تطور الحالة مع السماح
للعمود الفقري بمواصلة النمو والحفاظ على مرونته.
يُلجأ عادةً إلى هذا النهج في حالات الجنف المبكر
التدريجي عندما يكون انحناء العمود الفقري كبيراً،
وغالباً ما يتجاوز 40 درجة (مقاساً بزاوية كوب)،
كما هو موضح في العديد من الدراسات حول تقنية
تصحيح قمة الجذر النشط. كما تؤثر خصائص
الانحناء المحددة، مثل انحناء الفقرات عند القمة، على
قرار استخدام هذه التقنية.
تركز تقنية تصحيح قمة الجذر النشط على تصحيح
انحناء قمة العمود الفقري، وهي الجزء الأكثر انحناءً.
وتستخدم هذه التقنية غرسات متخصصة لتطبيق قوى
مضبوطة، تعمل على توجيه العمود الفقري تدريجياً
نحو استقامة أفضل مع مرور الوقت. وتُعد المتابعة
الدقيقة ضرورية لمراقبة استجابة النمو وسلوك انحناء
العمود الفقري.
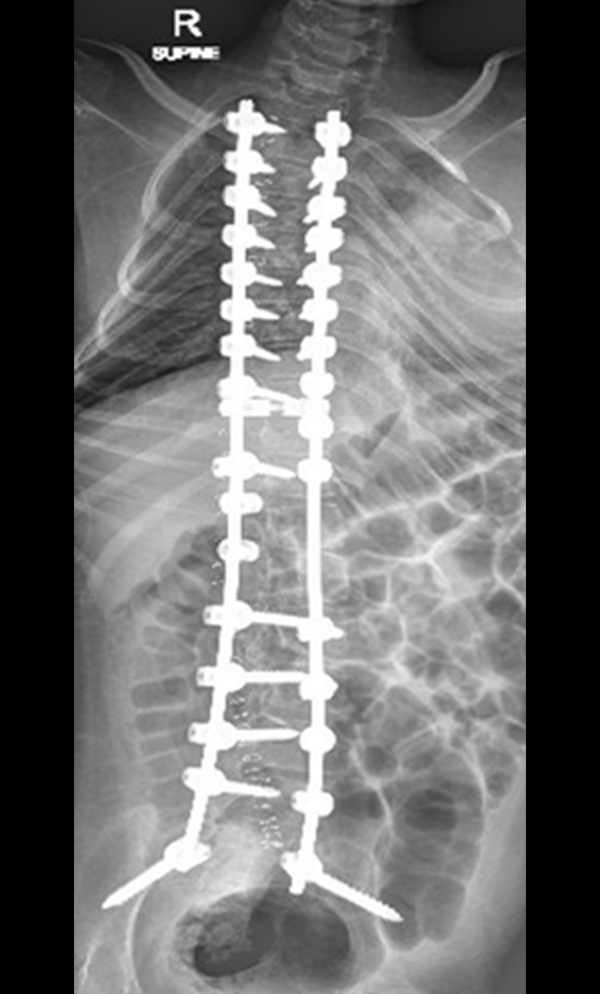
7. جراحة الجنف العصبي العضلي - عادةً ما تكون
الانحناءات متوسطة إلى شديدة / سريعة التطور
يرتبط الجنف العصبي العضلي بحالات عصبية أو
عضلية كامنة، وقد يتطور بوتيرة أسرع من الجنف
الطبيعي. يؤثر هذا التطور غالباً على توازن الجلوس،
والراحة، وآلية التنفس. يُنظر عادةً في التدخل
الجراحي عندما يصل انحناء العمود الفقري إلى
حوالي 40-50 درجة أو أكثر، خاصةً إذا كان
الانحناء متفاقماً أو يُسبب مشاكل وظيفية كبيرة. في
بعض حالات الجنف العصبي العضلي، قد يُوصى
بالجراحة في وقت أبكر، عند حوالي 20-40 درجة،
إذا كان الانحناء يتفاقم بسرعة ويؤثر على الأداء
اليومي للمريض.
تعتمد الجراحة غالباً على تصحيح الانحناء وتثبيت
العمود الفقري باستخدام براغٍ وقضبان معدنية
متخصصة لتحقيق الاستقرار طويل الأمد. وفي بعض
الحالات، قد يشمل التثبيت الحوض لضمان توازن
أفضل للجذع. يهدف هذا الإجراء الجراحي إلى
تحسين استقامة الجسم بشكل عام، والتوازن أثناء
الجلوس، وتلبية احتياجات الرعاية طويلة الأمد.
ونظراً للتعقيدات الطبية لهؤلاء المرضى، يُعدّ اتباع
نهج متعدد التخصصات أمراً ضرورياً في التخطيط
للتدخل الجراحي.
خيارات علاجية أخرى غير جراحية:
استخدام الدعامات - انحناءات خفيفة إلى متوسطة
(عادةً ما تكون حوالي 25-40 درجة)
بالنسبة للمرضى الذين لا يزالون في طور النمو
ولديهم انحناءات في هذا النطاق، قد يوصى باستخدام
الدعامة للمساعدة في إبطاء تطور الحالة ودعم
استقامة العمود الفقري.
- الدعامة تحت الإبط: منخفضة الارتفاع وتلبس تحت
الملابس؛ تستخدم عادة للعديد من انحناءات منتصف
العمود الفقري إلى أسفله.
- دعامة ميلووكي: تمتد للأعلى لتوفير دعم أوسع
للجذع والرقبة؛ تستخدم عندما تكون هناك حاجة إلى
تحكم أكثر شمولاً (غالباً لانحناءات العمود الفقري
العلوي).