A) Gradual limb lengthening and deformity correction
The procedure involves gradual limb lengthening and deformity correction by attaching an external fixator (unilateral or ring fixator) for the correction of the limb. The external fixators are fixed to the bones of the limb from outside with pins and wires. Another option for bone lengthening is using special nails implanted inside the bone in the medullary canal fixed with screws inside.
B) Epiphysiodesis
The proinciple of the surgery is to stop the growth of the bones at their growth plates. The surgery can be only performed on children whose bones are still growing. This procedure can be performed with special plates which can be removed after the limb length discrepancy is compensated and allows the growth plate to grow again. Another option is to to remove the growth plate which is a special cartilage completely for a permanent stopping of the growth at this bone end
c) Hemiepiphysiodesis
In this process, a temporary metal plate is attached to one side of the bone to halt its growth temporarily while the other side continues to grow. The surgery allows the deformed bone to straighten over time as the child grows. After the deformity is corrected the plate can be removed and the bone continues growing symmetrically
D) Acute deformity correction
This treatment involves the cutting and repositioning of bones with acute correction of the deformity. The bones are holding in corrected position by metal plates, rods, nails, wires, screws, nails or external fixators until the bone cut has healed. The deformity treatment is completed in a single surgery and doesn’t require any gradual correction. The fixation material will be removed after the bone has healed. However, not all deformities can be treated by this procedure as the nerves allow only a certain distraction before getting damaged. Therefore, to avoid nerve damage only small degrees of deformities can be corrected acutely
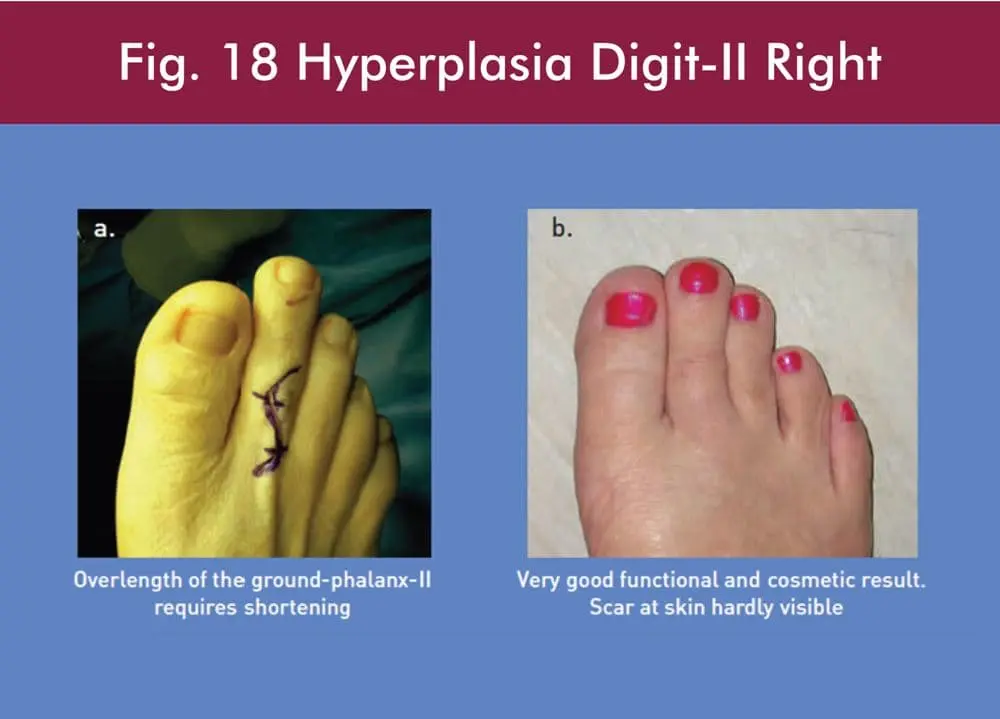
E) Limb shortening
Limb shortening as its name suggests is done by removing a segment of the longer bone. It can be performed in cases for limb length discrepancies of 1-4 cm.
Deformities : Deformity Correction
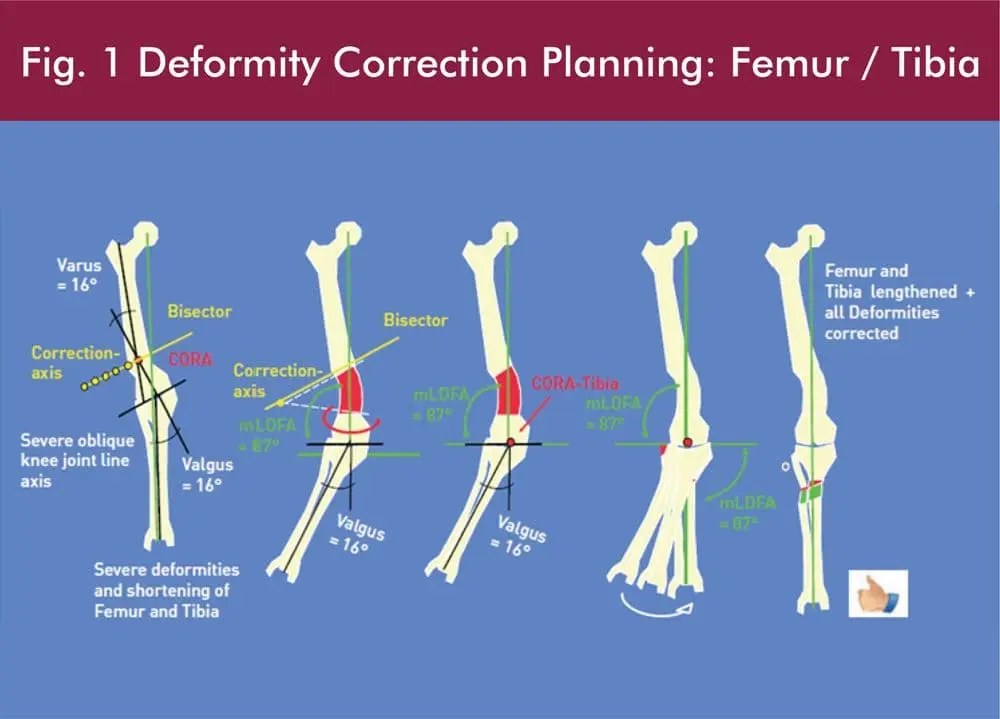
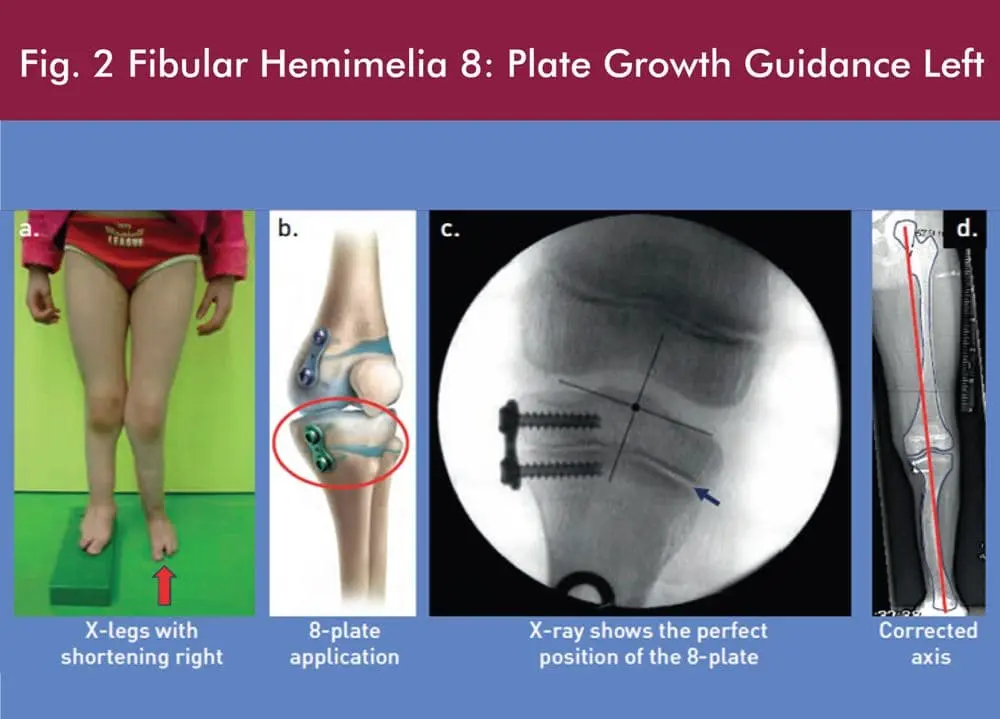
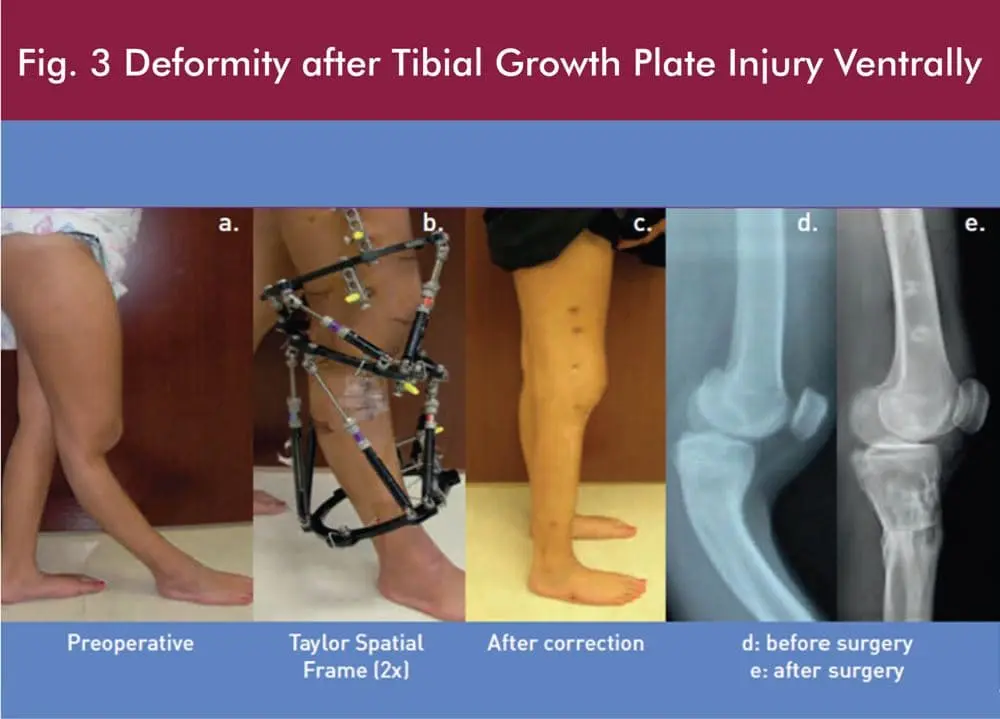
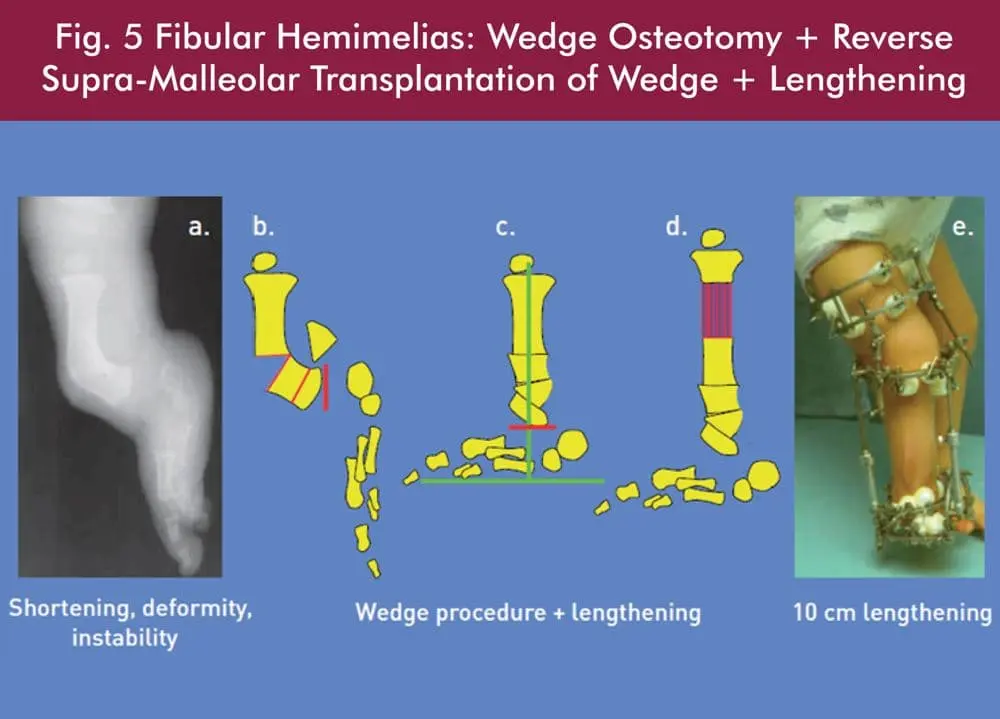
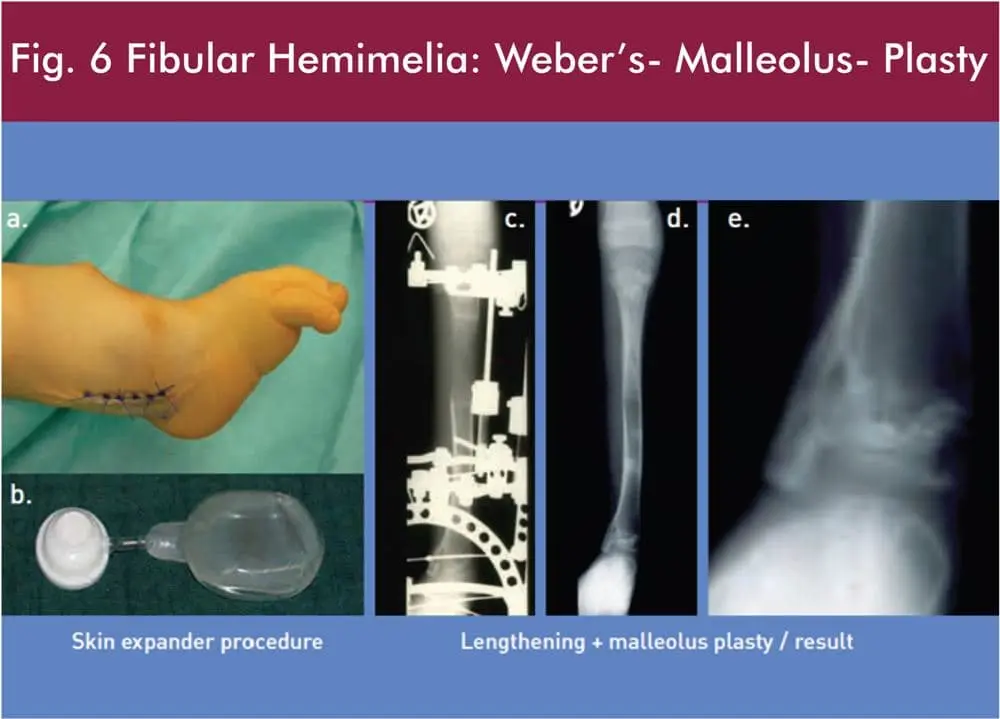
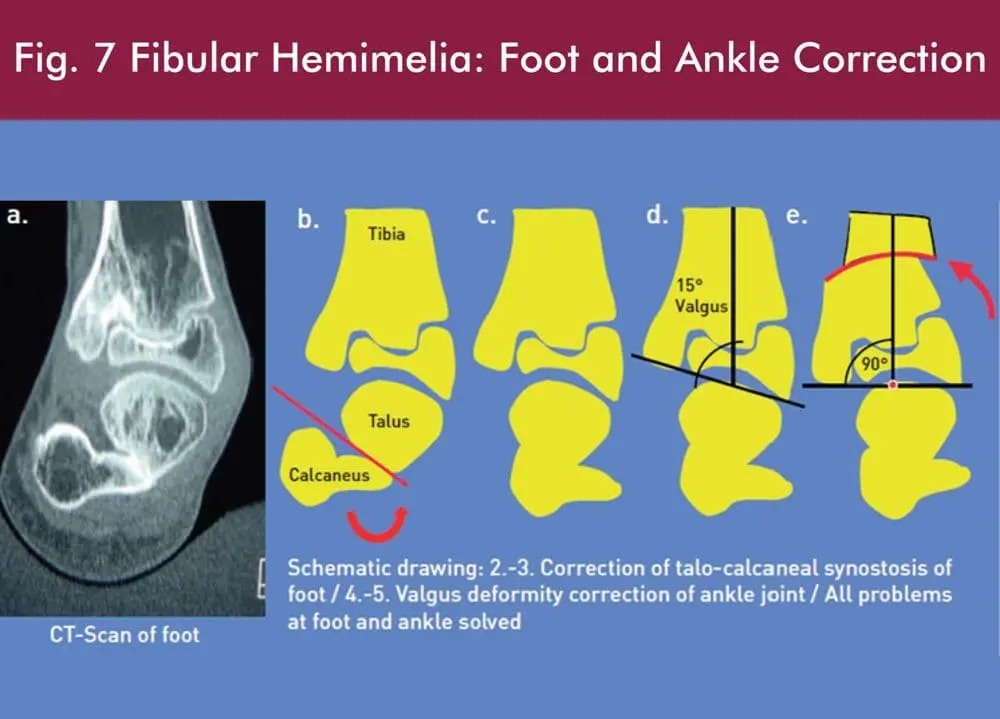
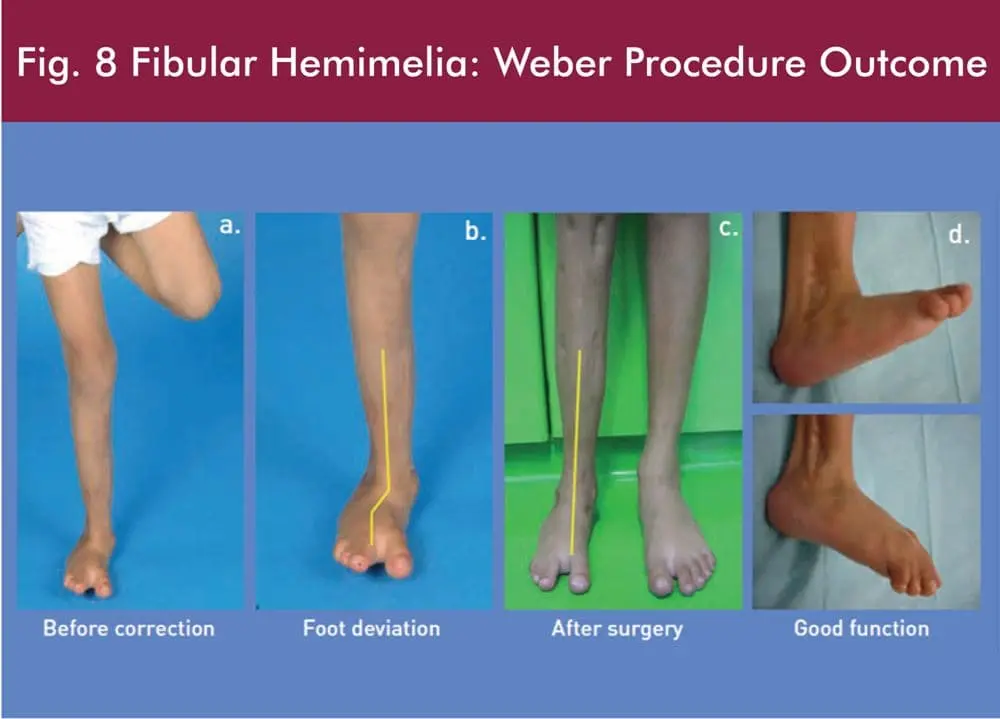
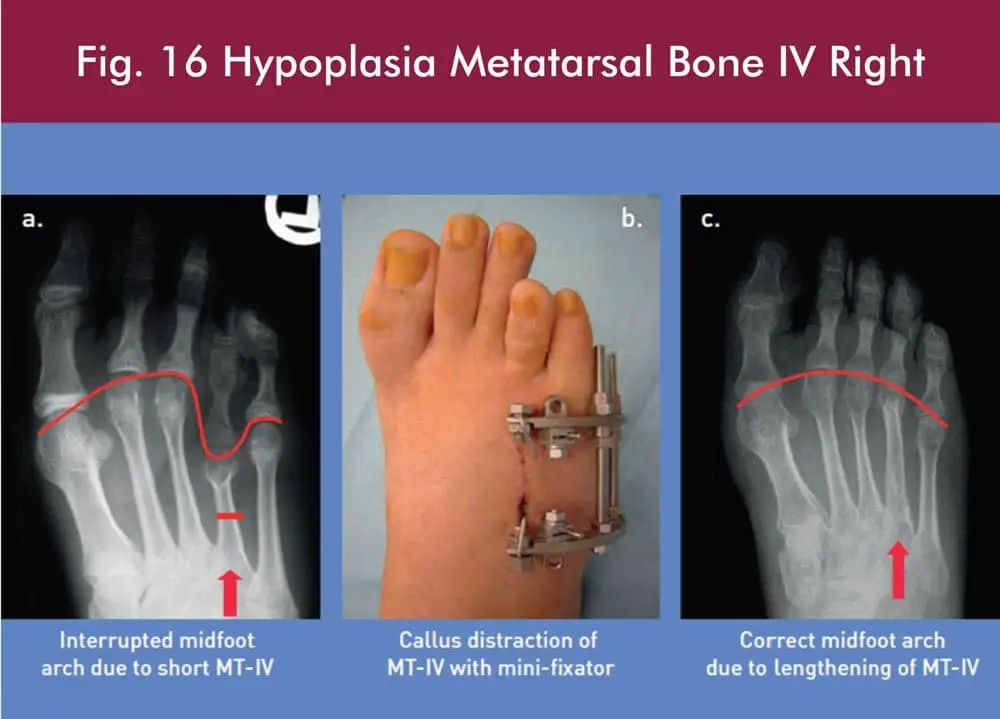
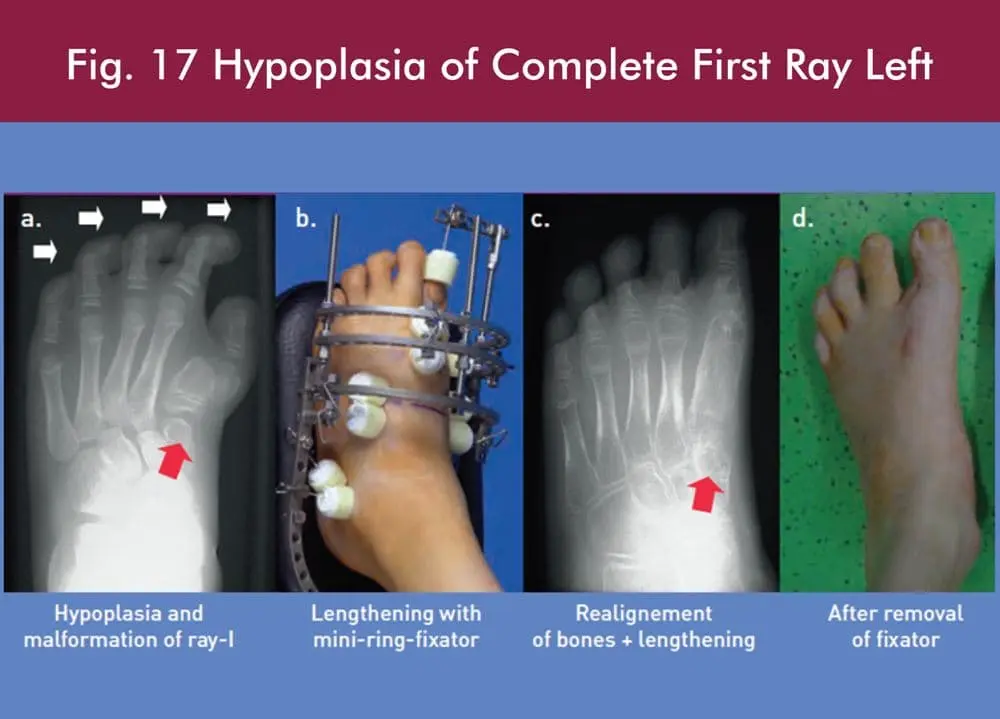
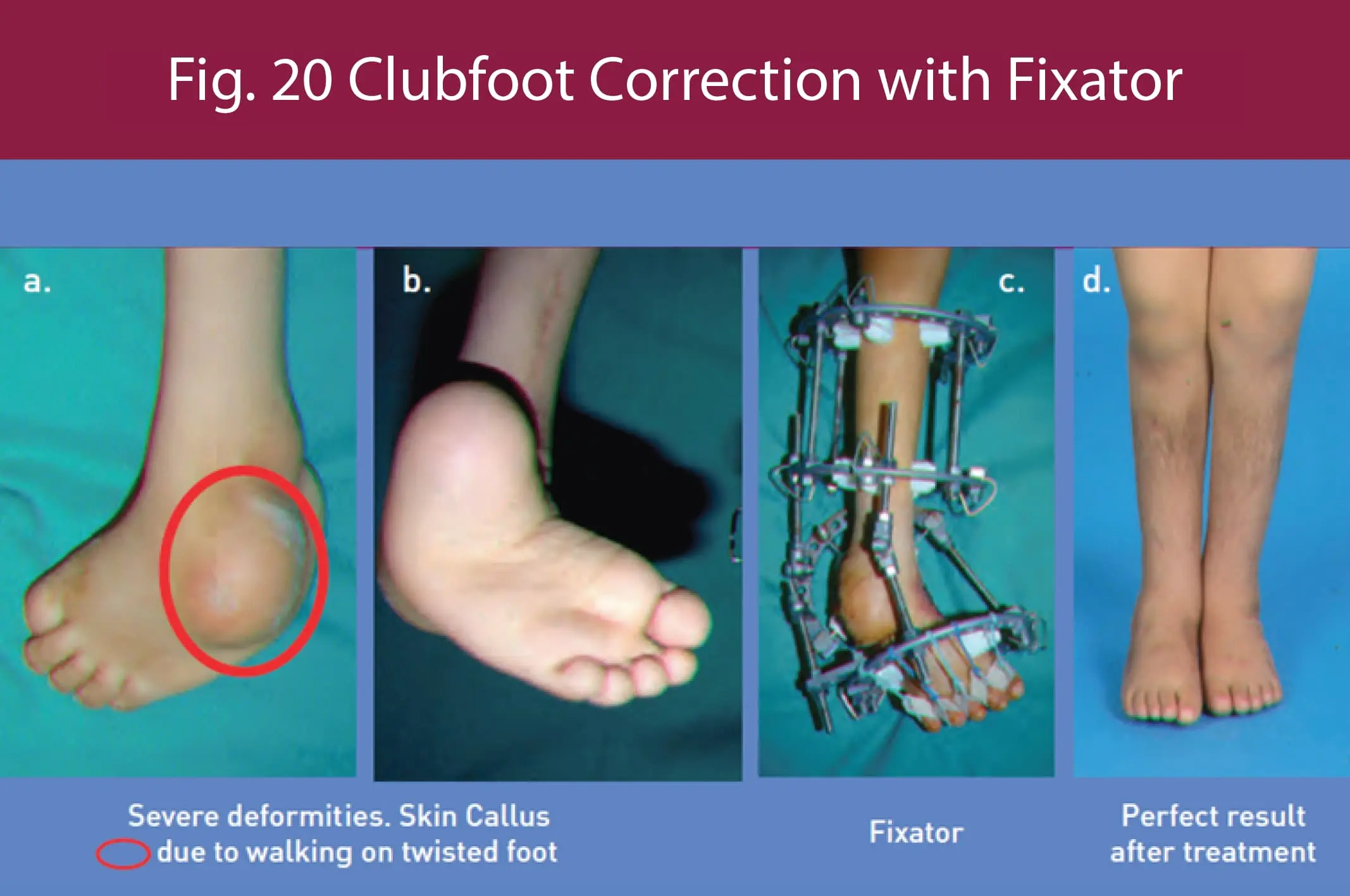
For correction of deformities a precisepre-operative deformity correction planning, experienced surgical performance and careful post-operative care are crucial. Minor deformity correction in children can be done by night brace, operatively with growth guidance, (8-plate, Fig. 2) and with acute correction of curved bones stabilized internally (plates, nail, rods etc.) or externally (fixators, Figs. 3, 5, 6 ,10, 11, 13, 14-17, 20).
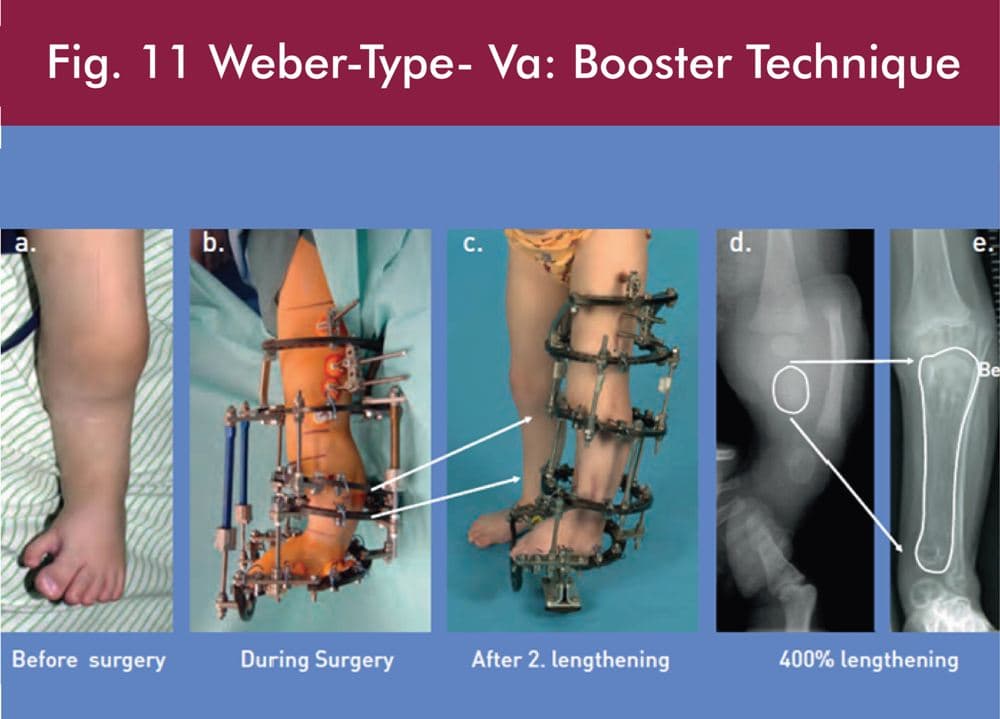
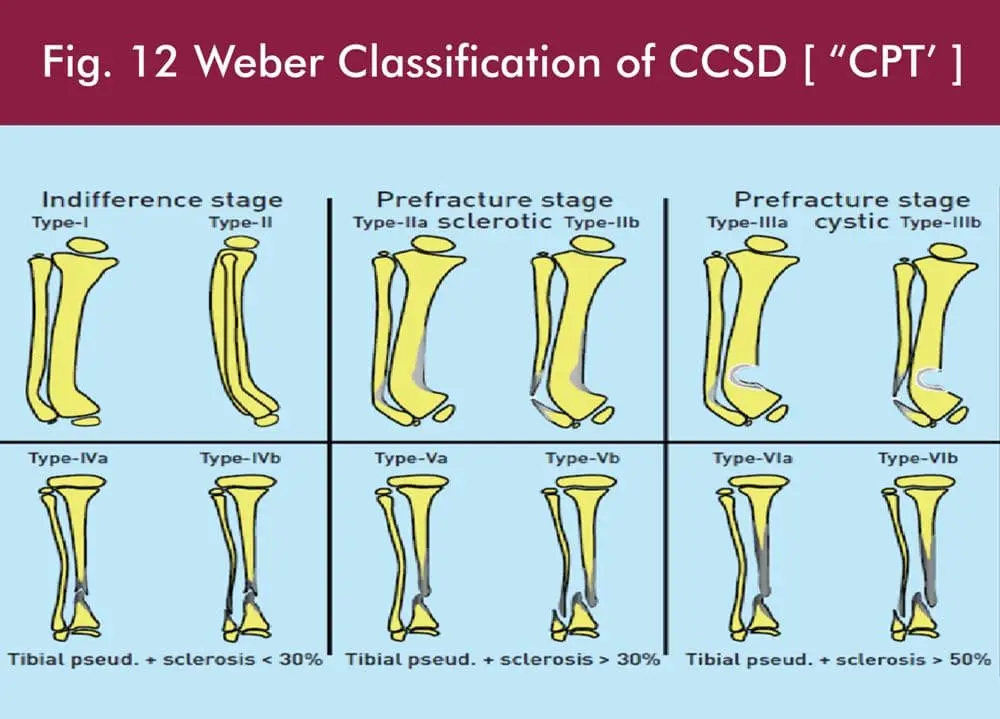
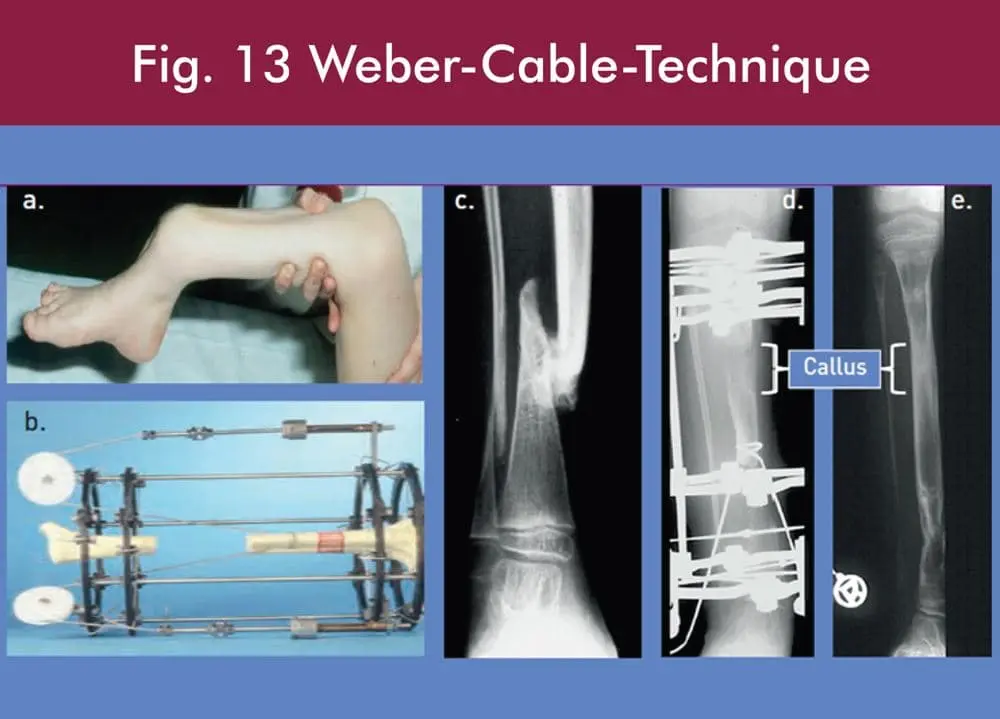
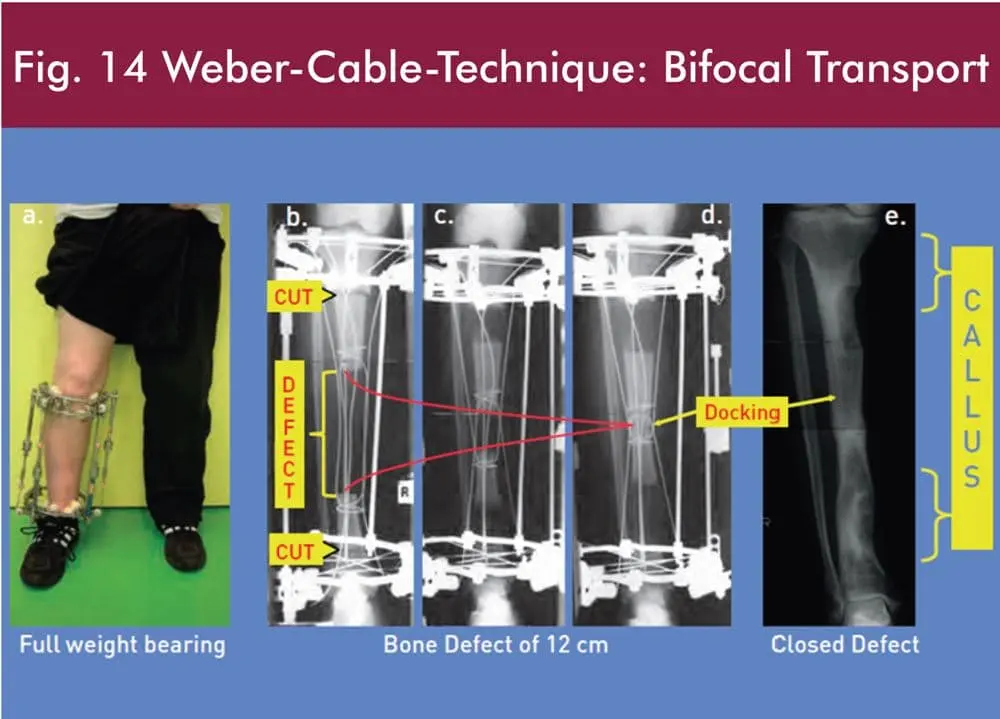
The congenital deformities and malformations are caused due to external disturbance of limb in the womb or genetic reasons. In major deformities, callus distraction has to be done with external and internal fixators.Complex deformities in combination with severe shortening demand a stable fixation with ring fixators [17]. The main principle of callus distraction is to apply man-made growth to a bone at the location where it is needed. Therefore, the bone has to be cut and the bone fragments have to be stabilized internally (lengthening nail) or externally (fixators).
After a couple of days, the cut bone fragments attempt to heal like in a fracture. This healing tissue is called callus. After several days, the callus is formed and due to its softness, it can be distracted. With a rate of approximately 1mm per day, the bone deformity can be corrected in all axis and additionally the short bone can be lengthened. The advantage of callus distraction is that with this continuous distraction the surrounding soft tissue (muscles, vessels, nerves, tendons etc.) is growing (like in a child). The distracted and growing callus maturates by time into full quality bone.
The two main reasons of deformities are congenital (figs. 2, 5-13, 16-20) and acquired (figs. 3,4,14,15),[6,7,19-22,24,25].The congenital deformities and malformations are due to external caused growth disturbances of limb(s) in the womb of the mother (e.g., breech position, lack of amnion fluid etc.) or genetic reasons and appear usually with multiple malformations of the whole limb. Prof. Weber found that the lack of amniotic fluid was related to the fetus developing limb and joint hip dysplasia and hip luxation. Prof. Dr Weber was honoured for his discovery and awarded for his Human Oligohydramnios-Sequence-Model for hip dysplasia and luxation at the 22 SICOT Conference in Sydney, Australia in 2002.
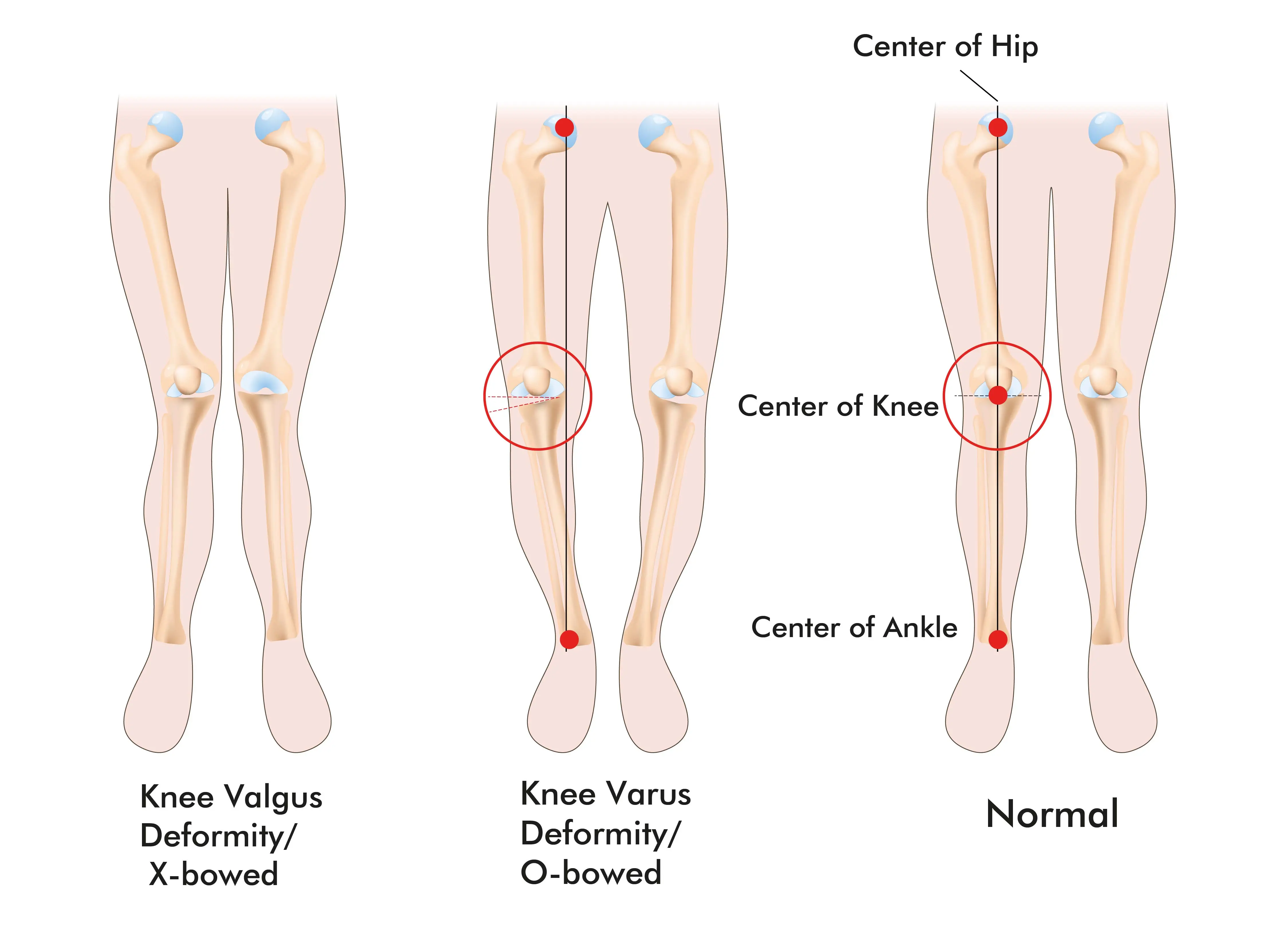
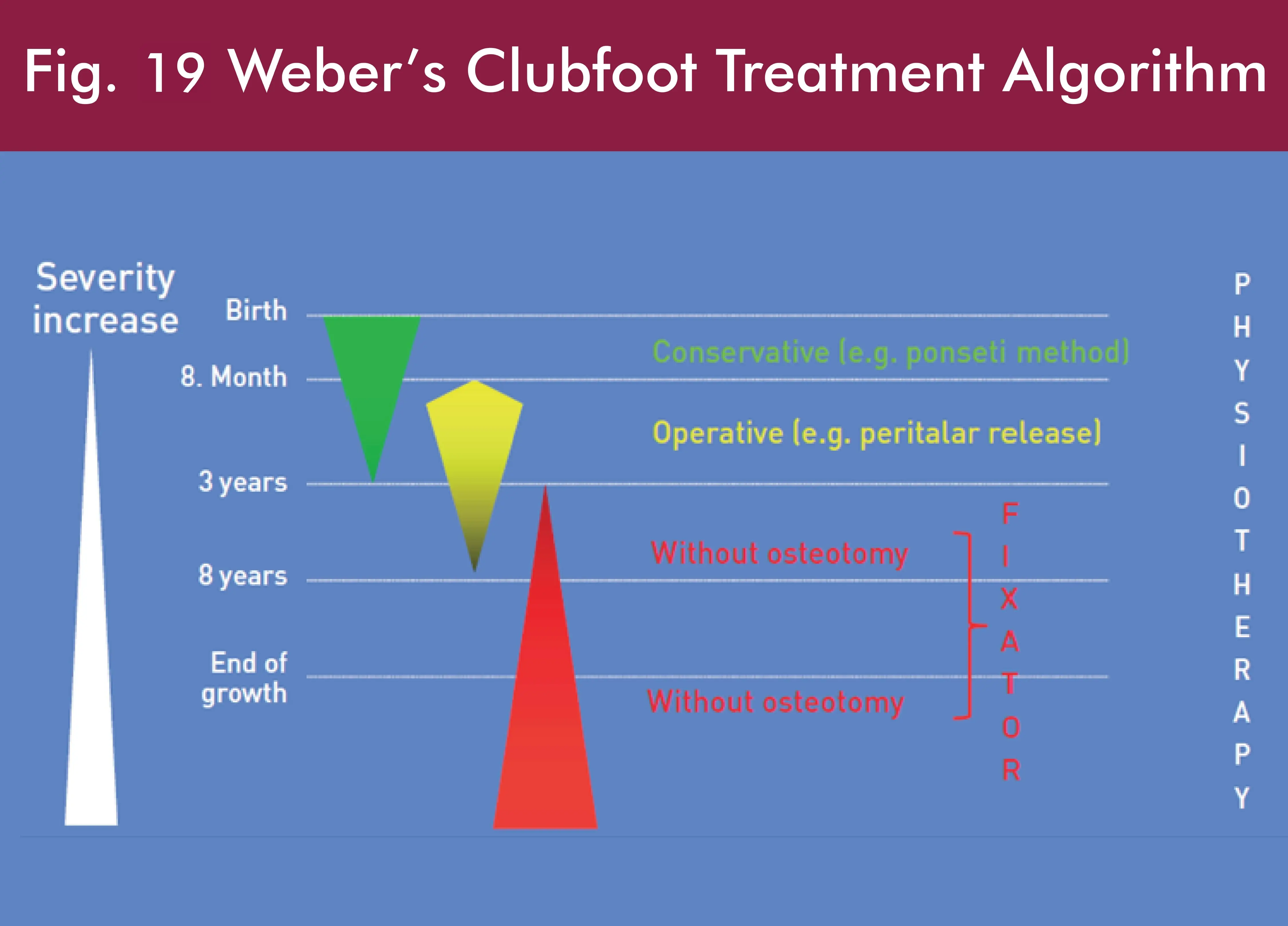
The acquired deformities are the result of incorrect fracture healing or damage to the growth plate, bone and joints in childhood due to injury, disturbance of the blood support, paralysis or spasticity of muscles or weakening of the bone due to Vitamin-D deficiency (very common in UAE) which can lead to the typical O or X-curved legs. In adult’s deformities occur mainly due to injuries of bone and joints with fracture healing problems like persisting deformities, delayed or non-union of the bones. Many adults also suffer from persisting deformities since childhood. In childhood, minor deformities can be treated conservatively with night braces or operatively with small surgeries using special plates for the guidance of growth at the growth plates. In major deformities or deformities with additional bone shortening, callus distraction has to be performed with external fixators or internal methods like lengthening nails. The following pictures are giving few examples of different reasons and techniques for the treatment of deformities, defects and malformations
Adam Vital is the best orthopaedic and sports medicine hospital with the best pediatric orthopaedic surgeon in Dubai. Our team of orthopaedic foot specialists and traumasurgeons will provide you with the best care and excellent treatment for all kinds of musculoskeletal problems including, limb lengthening and limb reconstruction.
References :
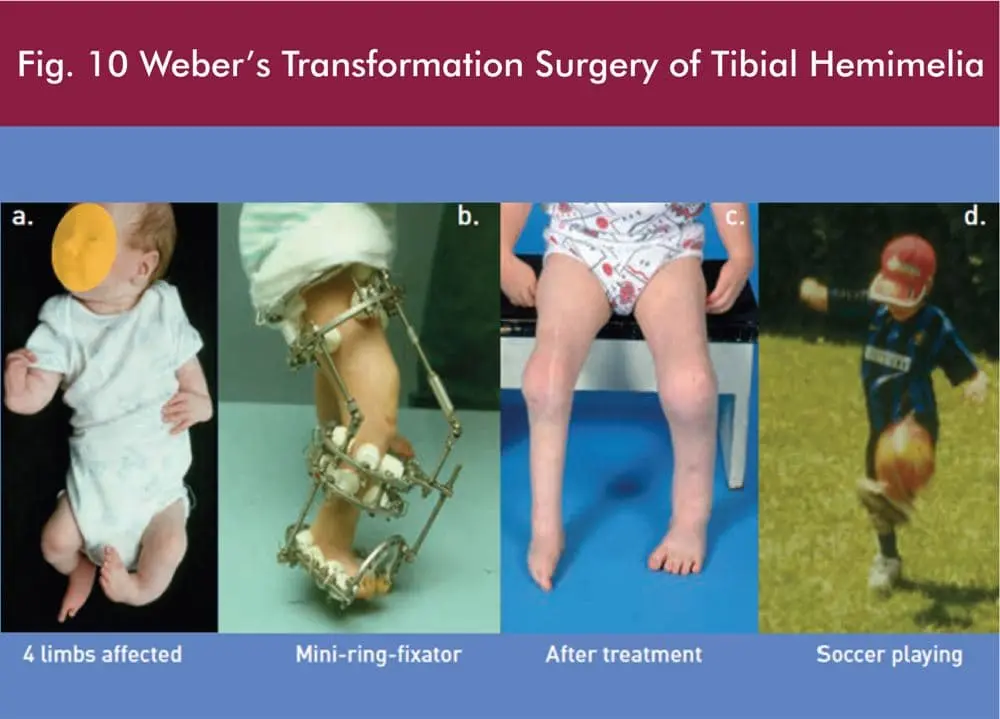
1. Weber, M.: Treatment of Tibial Hemimelia in M. Kocaoğlu et al. (eds.), Advanced Techniques in Limb Reconstruction Surgery, Springer Berlin Heidelberg, 2015
2. Weber, M.: Congenital Pseudarthrosis of the Tibia: Redefined (Congenital Crural Segmental Dysplasia) in M. Kocaoğlu et al. (eds.), Advanced Techniques in Limb Reconstruction Surgery, Springer, Berlin Heidelberg,2015
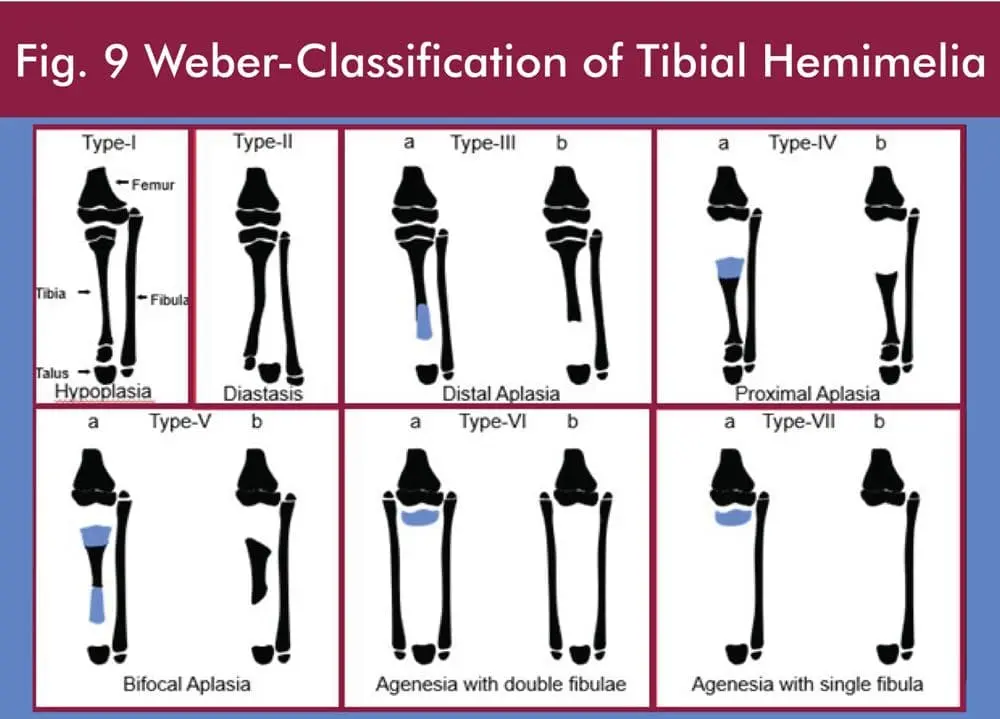
3. Weber M.: New classification and score for tibial hemimelia. J Child Orthop (2008) 2:169-175
4. Weber, M.: Congenital Leg Deformities: Tibial Hemimelia in S.R. Rozbruch and S. Ilizarov (eds.), Limb Lengthening and Reconstruction Surgery, Informa Healthcare, New York, 2007
5. Weber, M.: Congenital Pseudarthrosis of the Tibai. Redefined: Congenital Crural Segmental Dysplasia in S.R. Rozbruch and S. Ilizarov (eds.), Limb Lengthening and Reconstruction Surgery, Informa Healthcare, New York, 2007
6. Hermanns B., Senderek, J., Füzesi, L., Weber, M.: Periostal proliferations in bone lesions of congenital pseudarthrosis of the tibia have morphological features of neurofibromatosis type-I. Pathology in Research and Practice (2004)
7. Hermanns, B., Senderek, J., Klosterhalfen, B., Stemper, A., Büttner, R., Weber, M.: Malexpression of Hox c11 causes fibular a- or hypoplasia (FAH) in humans? Pediatr Dev Pathol (2004)
8. Weber, M.: Siebert, C.H., Goost, H., Johannisson, R., Wirtz, D.: Malleolus externus plasty for joint reconstruction in fibular aplasia: Preliminary report of a new technique. J PediatrOrthop (B) 11: 1-11 (2002)
9. Weber, M.: Neurovascular calcaneo-cutaneus pedicle graft for stump capping in congenital pseudarthrosis of the tibia: Preliminary report of a new technique. J PediatrOrthop (B) 11: 47-52 (2002)
10. Weber, M.: A new knee arthroplasty versus Brown´s procedure in congenital total absence of the tibia: A preliminary report. J PediatrOrthop (B) 11: 53-59 (2002)
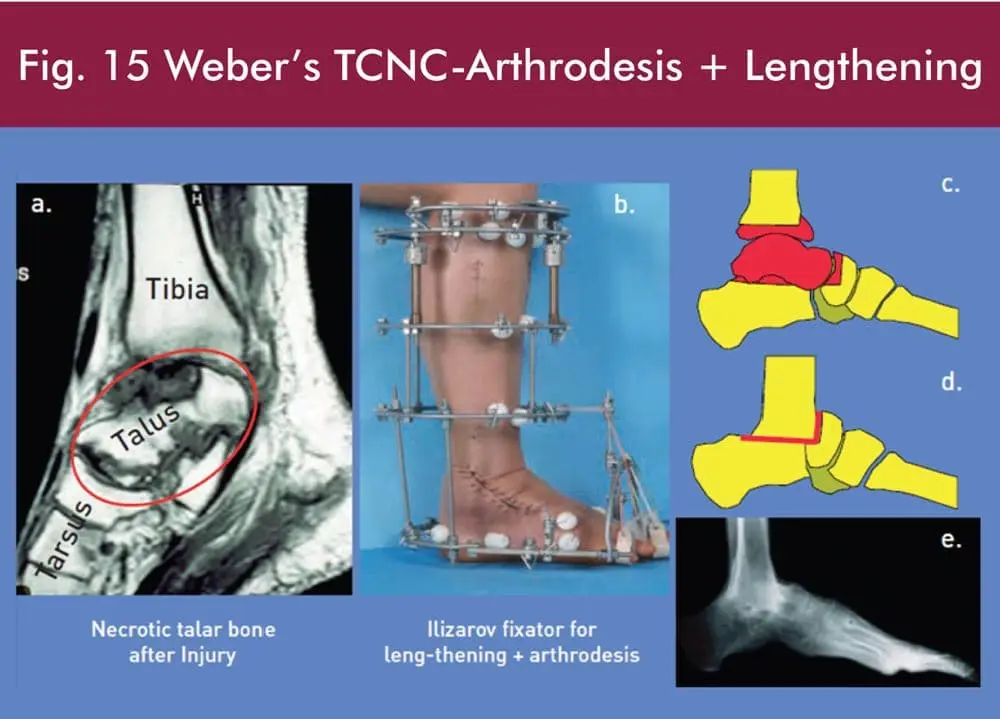
11. Weber, M., Schwer, H., Zilkens, K.W., Siebert, Ch.: The tibio-calcaneo-naciculo-cuboidale (TCNC) arthrodesis. - A new technique for treatment of difficult talar pathology -. Acta OrthopScand 73: 98-103 (2002)
12. Weber, M.: Eine neue Technik der Stumpfkappenplastik am Unterschenkel. Orthopädie – Technik 4:240-246 (2001)
13. Mahnken, A.H., Staatz, G., Hermanns, B., Gunther, R.W., Weber, M.: Congenital pseudarthrosis of the tibia in pediatric patients: MR Imaging. Am J Roentgenol 177: 1025-1029 (2001) 20
14. Weber, M., Schwer, H.: Der diabetischeFuß- Eine interdisziplinäreHerausforderung. Z Orthop 139: 54-55 (2001)
15. Weber, M., Siebert C.H., Heller, K.D., Birnbaum, K., Kaufmann, A.: Segmental transport utilizing cable wires and pulleys mounted on an Ilizarov frame – A new technique-. J Bone Joint Surg (Suppl.) 81-B: 148 (1999)
16. Weber, M., Schwer, E.H., Siebert, C.H.: FokussanierungeinerchronischsequestriertenTalusosteomyelitis durch die TCNC (tibio - calcaneo - naviculo - cuboidale) Arthrodese. Eine neue Technik am Ringfixateur. Unfallchirurg 102 402-405 (1999)
17. Schwer, E.H., Siebert, C.H., Kaufmann, A., Wilke, M., Weber, M.: Indication of change from unilateral to Ilizarov ring fixator. J Bone Joint Surg (Suppl.) 81-B: 148 (1999)
18. Weber, M.: Segmenttransport des KnochensmittelsKabelrollen und flexiblemDraht – Eineneue Technik am Ringfixateur-. Med Orth Tech 118: 134-140 (1998)
19. Weber, M.: Wenz, W., van Riel, A., Kaufmann, A., Graf, J.: Das Holt-OramSyndrom (HOS). – Literaturüberblick und aktuelleorthopädischeBehandlungskonzepte-Z Orthop 135: 368-375 (1997)
20. Axt, M. W., Niethard, F. U., Döderlein, L., Weber, M.: Principles of treatment of the upper extremity in arthrogryposis multiplex congenital type I. J PediatrOrthop (B) 6: 179-185 (1997)
21. Spranger, S., Weber, M., Tröger, J., Tariverdian, G., Opitz, J.M.: Bilateral radial deficiency with lower limb involvement. Am J Med Genet 63: 193-197 (1996)
22. Merkelbach, H., Carstens, C., Weber, M.: OrthopädischeProblemebeim Morbus Down. MonatsschrKinderheilkd 144: 778-785 (1996)
23. Weber, M.: Johannisson, R., Bos, I., Schröder, S., Rehder, H.: Oligohydramnios sequence as human morphological model of hip dysplasia and luxation. SICOT/SIROT XXII World Congress, 25.-30. August in San Diego, USA (Poster) Abstractbook: S. 583, P 1634 (2002)
24. F.U. Niethard, M. Weber, K.-D. Heller (eds.): Orthopaedie compact. Thieme, Stuttgart, New York, 2005
25. Rehder, H., Weber, M., Heyne, K., Lituania, M.: Fetal Pathology – Nonchromosomal in E.F. Gilbert, J.M. Opitz (eds.) Genetic Aspects of Developmental Pathology, Alan R. Liss, Inc., New York, 1987